For GP's

More Detailed Medical Information for Doctors
This page is directed at the medical profession, so do not be concerned if you don’t understand all the terminology! If you are interested in an explanation, do give us a call. We are always happy to run you through the medical terms.
Diagnosis of Infant Head Deformities
It is important to establish the cause of the head deformity first. This could be due to either synostotic or non-synostotic changes. The former are relatively rare, and they sometimes occur as part of syndromes. In these cases cranial sutures ossify prematurely, and further growth of the skull in the affected area is impossible. This can lead to unusual head shapes – some of them rather bizarre. Our surgeons are eminently qualified to diagnose these.
In contrast to this condition, there is no premature closure of cranial sutures in non-synostotic deformities, which are diagnosed much more frequently. These deformities usually occur through external influences. For example, birth related complications or changes due to the positioning of infants’ heads can result in a variety of deformities. Also, intrauterine restrictions e.g. in multiple births have been described as a cause.
Since 1994, many paediatric associations world-wide have been propagating back sleeping positioning as means of avoiding Sudden Infant Death Syndrome (SIDS). Positional Deformities have increased since. They account for the majority of head deformities. Muscular imbalances – predominantly in the neck area – occur in most cases; they are probably intensified by the one-sided positioning of heads. Even in the case of minor deformities, these muscular imbalances render a simple therapy of attempting to reposition the head impossible. Due to shortening of muscles in the neck (torticollis), forced positions may occur, which can be adverse to a symmetric growth of the skull. A shift of the skull base – visible in differently positioned ears or other asymmetries of the face – may be caused by harmful sleeping positions.
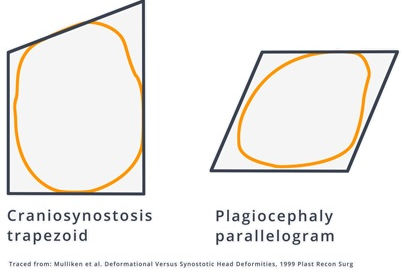
An asymmetric growth of the skull base and face may have negative bearings on mandibular growth. In most cases these visible deformities make it possible to diagnose without resorting to invasive or radiological examinations. Thus non-synostotic deformities due to the positioning of infants´ heads – looked at from a “birds eye view” – appear shifted in a parallelogrammatic fashion. In contrast to this, the deformity caused by prematurely ossified cranial sutures often appears trapezoid.
Therapy of Infant Skull Deformities
After the diagnosis of a premature ossification (synostosis), an early operative correction is indicated. This facilitates normal brain growth, and aesthetic aspects are corrected too.
But when cranial bones shift without premature ossification, an alteration in the positioning of the infant’s head can result in a correction of the deformity in less severe cases (if applied before 6 months of age).
In cases of more severe deformities, which have already resulted in an asymmetry of the skull base, physiotherapy is indicated. Additionally, therapy with an orthotic headband may be appropriate.
This treatment makes use of the natural growth of the infant’s head, which is at its maximum in the first year of life. The correction of head deformities in this way does not work by pressuring prominent areas of the head.
Rather, the flattened parts are allowed to expand through their own growth. The so-called head orthesis (or helmet) is constructed in such a way so as to suppress the growth of the prominent areas for a time until the growth of the flattened parts has caught up.
It has been shown repeatedly that a child’s overall head growth is not restricted during helmet therapy, but follows the course of the original growth curve (percentile curve).
This therapy makes it possible to treat widely-varying deformities, and it has been shown that once a correction has been achieved at a young age, it remains stable for life.
This method is by no means new but was already known in antiquity, e.g. to the Egyptians, who aimed at reaching fashionable beauty ideals by bandaging their children’s heads accordingly.
Today, new materials are available, which render such treatment less complicated and less inconvenient for children. As maximum head growth only occurs in the first 18 months of life, headband treatment only makes sense during this period. Early treatment is therefore essential.
The optimum start age is 4 to 5 months. With moderate deformities, repositioning the infant and physiotherapy may be sufficient. If these methods fail, or in severe deformities with skull-base shift, an orthotic headband should be fitted to reach satisfying results. Thus, non-operative treatment is effective, and corrective surgery can be avoided in later life.
Please note that treatment options and success of treatment depend on many different factors and outcome might vary from patient to patient. Please do contact our surgeons for a face to face assessment.
An further illustration can be found on the second page of this article.